Pathology Consultative Services – Head & Neck
Thyroid Grossing Guidelines
Based on Cleveland Clinic best practices, these guidelines enable high quality patient care while conserving resources, supporting timely diagnoses, and realizing cost savings within the laboratory.
Our grossing practices for thyroidectomy cases include submitting an average of eight blocks per thyroidectomy, alleviating unnecessary burdens to staff and reducing costs while maintaining high-quality supporting services.
Additionally, this grossing protocol includes a templated gross description that simplifies grossing, making it easier for the pathologist to identify the most significant nodules and complete synoptic reports.
Thyroid Grossing Manual & Gross Description Template
Overview
Chart review must be performed to obtain:
- Indication for surgery
- Ultrasound report
- Any prior cytology aspirate specimens
- and any available molecular testing results (i.e. Afirma or Thyroseq)
Grossly identified discrete lesions must be clearly described and designated to allow histologic sections to be correlated with each lesion.
A discrete lesion may be a solid, fleshy nodule or an irregular, tan-white scarred area. The normal background parenchyma is tan-red and homogenous; however, sometimes the background thyroid parenchyma will be diffusely nodular as in multinodular goiter. It is imperative to recognize discrete lesions that look different from the colloid filled nodules of multinodular goiter.
Gross evidence of invasion is important.
Invasion into surrounding tissue outside the thyroid is required for staging – if present, document and photograph.
Encapsulation is important.
When present, carefully evaluate the capsule for invasion. Gross assessment of encapsulation is not always accurate but should be attempted.
Multinodular Goiters
If there appears to be more than three (3) discrete lesions in a thyroid, it is likely a misinterpretation of multinodular goiter.
Submission Guidelines
Indication for Surgery
Number of Blocks to Submit
Notes
Normal
Graves
Hashimoto’s
(NO Discrete Lesion)
Two (2) blocks
One (1) block per lobe
Multinodular Goiter
Five (5) blocks
Two (2) blocks per lobe, one (1) block of isthmus
History of Multiple Endocrine Neoplasia (MEN)
Family History of Medullary Carcinoma (prophylactic thyroidectomy)
Five (5) blocks
Two (2) blocks per lobe, one (1) block of isthmus
Completion Thyroidectomy for Recent Carcinoma on Partial Thyroidectomy
One (1) block if there is no discrete lesion
If a gross nodule is present, gross per Cleveland Clinic guidelines.
Infiltrative or Unencapsulated Discrete Lesion
Lesion is ≤2 cm: Submit entire specimen
Lesion is > 2 cm: One (1) block per cm
Focus sampling to identify invasion and any extension into skeletal muscles or other extrathyroidal structures.
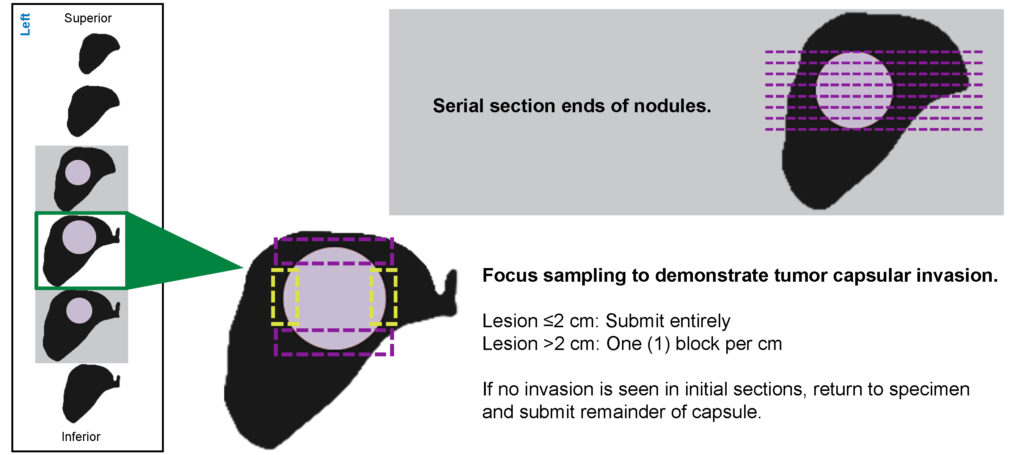
Encapsulated Discrete Lesion
Lesion is ≤2 cm: Submit entire specimen
Lesion is > 2 cm: One (1) block per cm
Focus sampling to demonstrate tumor capsule invasion.
Thyroid Grossing Steps
1. Perform clinical review
a. Identify indication for surgery (nodule vs goiter vs Graves etc).
b. Review ultrasound to correlate clinically with the gross assessment.
c. Review prior FNA reports and molecular testing if available.
2. Orient specimen
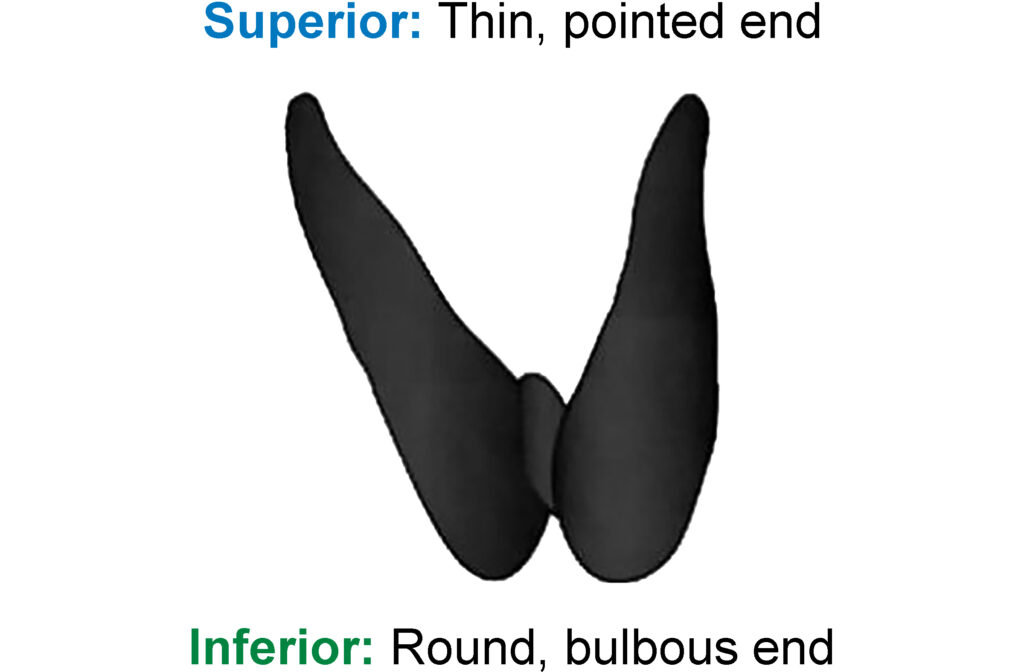
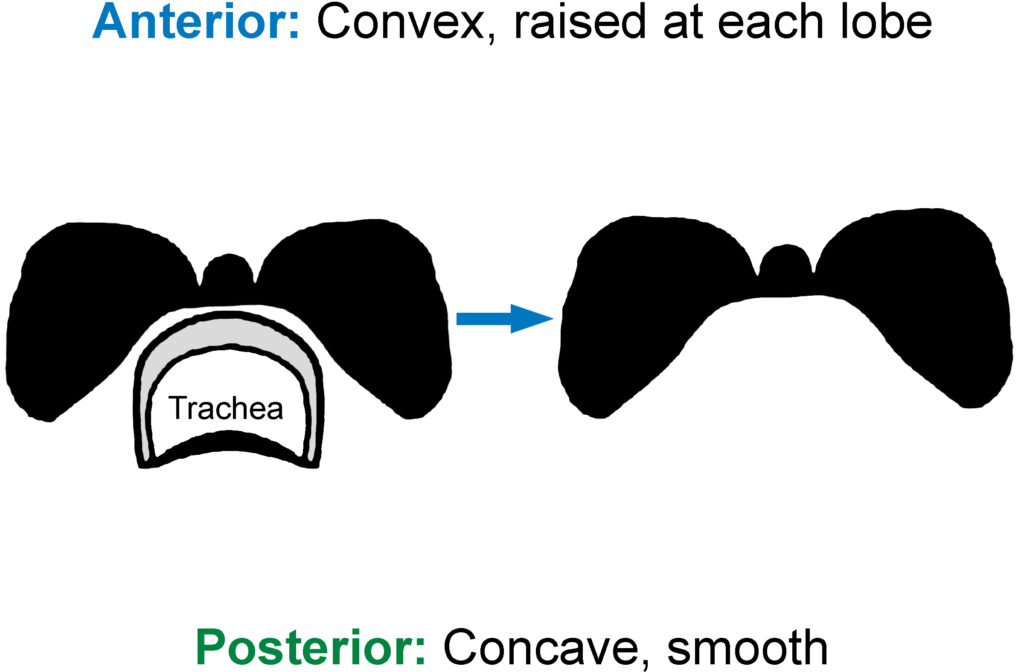
3. Examine
If available, correlate with the operative report for the presence of attached structures such as skeletal muscle, large nerve or vascular structures, and/or level VI lymph nodes.
4. Record weight in grams
5. Measure
- Overall specimen
- Right lobe
- Left lobe
- Isthmus in three dimensions
6. Ink outer surfaces
For all lobectomy or hemithyroidectomy specimens:
- Outer surface of lobe AND isthmus – blue or black
- Cut surface of isthmus – orange
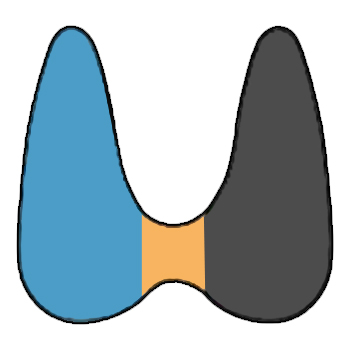
For intact total thyroidectomies:
- Outer surface of right lobe – black
- Outer surface of left lobe – blue
- Outer surface of the isthmus (if identifiable) – orange
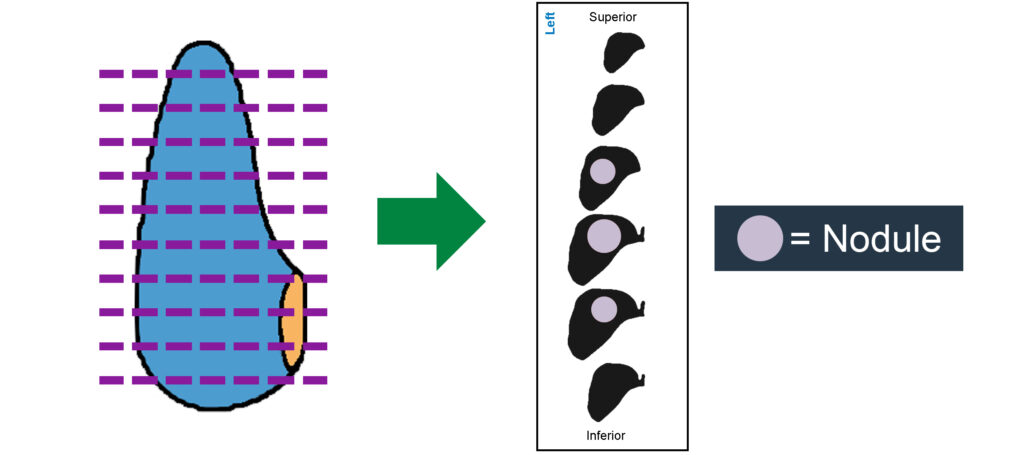
7. Section thyroid
For all lobectomy or hemithyroidectomy specimens:
- Serial section transversely from superior to inferior.
- Layout all sections on a damp paper towel to evaluate nodules (label towel as shown for preserving orientation).
For intact total thyroidectomies:
- Separate lobes from isthmus.
- Section lobes transversely & isthmus sagittally.
- Layout all sections on a damp paper towel to allow evaluation of nodules (label towel as shown for preserving orientation).

8. Evaluate and describe discrete lesions
- Number lesions sequentially (1, 2, 3…).
- Indicate location (left, right, or isthmus; superior, mid, or inferior pole).
- Measure each lesion in three dimensions.
- Describe: Encapsulation, border, color, consistency, etc.
9. Submit specimen as indicated
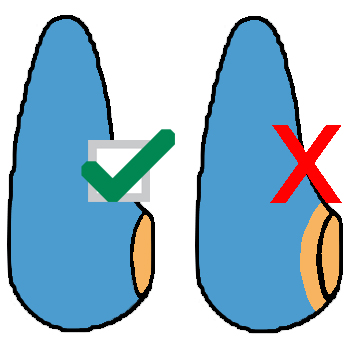
- For encapsulated nodules, submit sections as demonstrated below.
- When submitting nodules, ensure the cassette code indicates the nodule number and laterality. Always indicate if the nodule is representatively or entirely submitted.
- For central neck contents/lymph nodes – identify lymph nodes if possible and submit. Submit all remaining adipose tissue.
- Following submission of sections, ensure labeling of orientation and nodules on paper towels and carefully wrap residual tissue such that each nodule can be re-identified if additional tissue needs to be submitted.
Sectioning & Submitting an Encapsulated Nodule:

Thyroid Gross Description Template
Labeled:
[***]
Received:
[Fresh or Frozen]
Specimen Type:
[Total thyroidectomy, Hemithyroidectomy, Lobectomy, or Completion thyroidectomy]
Oriented:
[Yes or No]
(if yes, describe)
Weight:
[ ] grams
Size:
Overall: [in three dimensions] cm
Right lobe: [in three dimensions] cm
Left lobe: [in three dimensions] cm
Isthmus: [in three dimensions] cm
Pyramidal lobe: [in three dimensions] cm (if present)
Ink code:
– Black: External surface of the right lobe
– Blue: External surface of the left lobe
– Orange: External surface or resection margin of isthmus
Sectioning:
The [right and/or left lobes] are serially sectioned from superior to inferior. [The isthmus is serially sectioned from right to left.]
Number of discrete nodules:
[***]
Nodule
[#] (repeat for each discrete nodule, numbering 1, 2, etc)
Location:
[Right lobe, Left lobe, or Isthmus] and [upper, mid, or lower pole]
Size:
[in 3 dimensions] cm
Description:
[e.g. solid, cystic, color, calcification, circumscription, encapsulation, consistency] (if the nodule is encapsulated, remember to submit the entire capsule)
Gross extrathyroidal extension:
[Yes or No]
Background thyroid parenchyma:
[Describe]
Attached skeletal muscle:
[Yes or Not identified]
Attached lymph nodes:
[Yes or Not identified]
(if yes – number, location, range of size)
Attached parathyroid:
[Yes or Not identified]
(if yes – number, location, size)
Cassette Code:
[Indicate nodule number and lobe location for each cassette and if nodules are entirely submitted]
Approach to Thyroid Nodule Evaluation
Cleveland Clinic Laboratories approaches most thyroid nodules by considering the molecular basis for thyroid neoplasia, even in the absence of prior molecular studies.
Specifically, BRAF-like tumors can generally be distinguished from RAS-like tumors and non-neoplastic nodules when cytologic, gross, and histologic features are considered.
The table below highlights the key distinctions between BRAF-like and RAS-like tumors. At the time of gross evaluation and prior to section selection, consideration of cytologic, molecular, and gross nodule morphology can give a clue to the type of tumor being evaluated and guide the number of sections submitted.
BRAF-like Tumors
RAS-like Tumors
Typical Bethesda Cytology Categorization
– Suspicious for PTC (V)
– Positive for PTC (VI)
– Atypia of Undetermined Significance (AUS; III)
– Follicular Neoplasm (IV)
Common Molecular Profiles
– BRAF V600E
– RET fusions
– BRAF fusions
– ALK fusions
– NTRK fusions
– NRAS, HRAS, or KRAS mutations
– BRAF K601E
– PPARG fusions
– THADA fusions
Gross Features
– Infiltrative irregular border
– Encapsulated/circumscribed
Best Approach for Sampling
– Representative sections to document staging parameters and diagnosis
– Initial representative sections to document invasiveness and diagnosis
– Additional sampling only if invasion is not identified in the initial sections
Histologic Features
– Well-developed nuclear features
– Infiltrative
– Papillary architecture
– Subtle nuclear features
– Encapsulated/circumscribed +/- invasion
– Follicular with possible hyperplastic appearance
Typical Histologic Tumor Types
– Conventional PTC
– Tall cell variant PTC
– Encapsulated follicular variant PTC
– Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP)
– Follicular carcinoma
– Follicular adenoma